|
� |
| |
Information | |
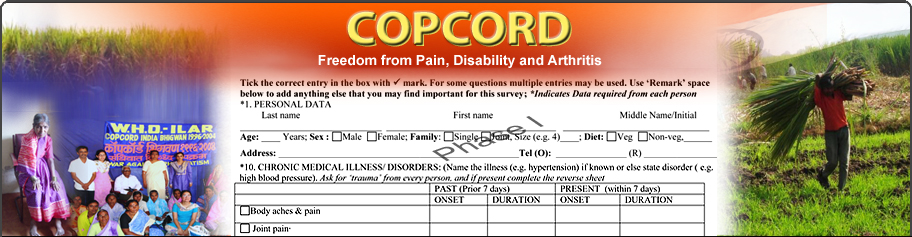
The
acronym COPCORD stands for community oriented program for control of rheumatic
diseases. The key operative words are community and rheumatic diseases. COPCORD
is primarily an ILAR (International League of Associations for Rheumatology) initiative
which was launched in collaboration with WHO in late 1980s to gather data on pain
and disability with a focus on grass root developing economies. The program was
meant to measure and evaluate pain and disability in rheumatic disorders.
COPCORD was to fill the void in the realm of data on rheumatic and allied
musculoskeletal disorders (RMSK) in the developing World. In this regard, it has
been an outstanding program for community aches and pains. Several COPCORD surveys
all over the World have highlighted the RMSK burden and its impact and outcome.
The active and enthusiastic participation of community and its health care providers
to complete COPCORD surveys has been overwhelmingly satisfactory and endearing.
Though the second C in COPCORD represents control, COPCORD was not envisaged
as a public health initiative. Control of rheumatic diseases is a major challenge
for public health. Though COPCORD has imparted health education in several communities,
the thrust has rarely if ever been on control (or prevention). But there is sufficient
data gathered by several COPCORD surveys to lay a foundation for prevention and
control strategies.
COPCORD was born out of a simple need to measure
RMSK pain and disability in a community. And the first item of the COPCORD
agenda all over the World has been to complete a community survey with motivated
grass root rheumatology oriented doctors using a low cost basic infrastructure
model. Though an epidemiology program, COPCORD is not bound by conservative and
rigid epidemiology tenets. It has been a program evolved in the field using clinical
senses and practical knowledge. Most of the investigators have been clinicians
with hardly any formal training in epidemiology and statistics. Largely, COPCORD
has been a nongovernmental project using local resources and funds. Principle
investigators have volunteered their time and expertise without any remuneration
or compensation. The doctors have used a uniform protocol and design to complete
the survey. Though several regional issues have dictated certain modifications
and further validation, the core questionnaires have uniformly captured the data.
Much of COPCORD surveys are published in peer
reviewed literature.
Though a data acquisition exercise, COPCORD
has also provided free of cost rheumatology services to the community in some
sites. Though mostly a onetime survey, COPCORD has continued beyond survey in
a planned manner in some sites to gather data on risk factors and incidence. The
program site and its results have often been endorsed by the respective Government.
Also, The Bone
and Joint Decade 2000-2010 national action network in India adopted COPCORD
to gather RMSK data.
Begun in Philippines under chaotic political conditions
in late nineteen eighties, COPCORD has successfully overcome several hurdles in
demonstrating MSK disorders in several countries in Asia and Latin America. Recently,
it has completed survey in Egypt.
 History
& Evolution History
& Evolution | |
COPCORD was launched by WHO (World Health Organization)
and ILAR (International League of Associations for Rheumatology) in 1980s. COPCORD
was designed as a low cost - low infrastructure local resources based community
program. The emphasis in population surveys was to record symptoms (in particular
pain and disability) rather than diseases and syndromes. Clinical and field epidemiological
skills rather than elaborate investigation was the basis of diagnostic approach.
In the parent COPCORD model , population data (Stage I) was collected
through three successive phases- house to house survey by a local health worker
to identify cases (Phase I), interview based questionnaires by paramedics to capture
pain and disability (Phase II), and a standard medical evaluation by a doctor
with some training in rheumatology(Phase III). A validated core questionnaire
(CCQ), developed initially by ILAR could be modified to suit the local requirements
as far as the principle questions on pain and disability were unchanged. Later,
in the Bhigwan (India) COPCORD a fast track model was devised wherein all the
three phases of Stage I were conducted in parallel and the CCQ contained a more
comprehensive capture of pain and quality of life.
COPCORD also advocates
education of the community and health care providers and identification of risk
factors (Stage II). Based on community data, it also encourages investigators
to plan, execute, and maintain improved health care through preventive and control
strategies (Stage III). However, very few COPCORD were continued beyond the initial
survey. The Chinese COPCORD has pursued several population studies on knee pains
and osteoarthritis to identify risk factors. The Indonesian COPCORD survey findings
of significant gout in the community led to several long term national initiatives
in the nineties. Bangladesh COPCORD was continued further to evaluate low back
ache and knee pains. The Bhigwan (India) follow up program (Stages II and III)
has been the longest continuing COPCORD and is currently in its 15th year.
The earlier versions of COPCORD Core Questionnaire (CCQ) were based on ILAR
experience [HA
Valkenburg (The Netherland), Richard
Wigley (New Zealand), KD
Muirden (Australia), & others). The CCQ was later modified and developed [APLAR
COPCORD Workshop Korea,1991, Prof
S. van der Linden (The Netherlands), Late
John Darmawan (Indonesia), and others). Maintaining basic framework, CCQ was
modified and further developed by the fast track COPCORD Bhigwan (India) model
and published (APLAR J Rheumatol 1997; 1: 145-154). The current proposed CCQ is
based on the latter experience, review at the WHO-ILAR BJD Meeting Vienna, Austria
2005 (Clin Rheumatol 2007; 26: 1217-1227), inputs from several COPCORD investigators
and experts, and discussions in the APLAR 2006 (Kuala Lumpur) COPCORD Session
(Dr. Arvind Chopra,
India, and others).
The WHO & UN supported The Bone
& Joint Decade (BJD) 2000 2010 has included trauma along with arthritis
& osteoporosis amongst the disease target conditions. The BJD program aims to
create awareness and empower patients. It will measure the burden of rheumatic
and other musculoskeletal disorders and reduce it in time through various community
and medical programs. The new CCQ has incorporated
a section to capture data on trauma.
The populations in COPCORD have
generally been selected non-randomly. However, some randomized techniques were
used in China (Shangai, Shantou), Peru , Brazil, Chile Mexico, Kuwait and Lebanon
. Different personnel (doctors, nurses, health workers, volunteers, etc) have
collected data. The earlier COPCORD used CCQ based on very early experience .
Later, it was made less cumbersome. However, the survey screening Qs was generally
meant to identify pain/swelling/stiffness and limited range of motion in joints
and/or musculoskeletal soft tissues in the last seven days (current) and/or anytime
in the past. Pain was predominantly captured. But methods of recording pain have
differed. COPCORD surveys in India , Malaysia , Peru and Australian Aborigines
used a human mannequin to record pain. Some of the earlier COPCORD surveys have
published rates of joint pain/rheumatic disorders/ rheumatism (Beijing & Shantou
ILAR China , Pakistan , Indonesia ). Patients with history of trauma prior to
chronic MSK were excluded (China, Peru, Brazil , Iran, and Kuwait).Disability
was recorded by asking specific individual items or using a validated modified
Stanford Health Assessment Questionnaire (HAQ) as in India. Brazil COPCORD used
a SF-36 quality of life instrument. Several countries have completed COPCORD surveys
in both urban and rural regions. China,
India and
Mexico have completed COPCORD surveys in several sites.
The COPCORD
sample size was not meant to measure uncommon disorders like lupus. Some earlier
COPCORD surveys took long periods for completion. In Stage I, Phases I & II were
sometimes combined . The response rate in various COPCORD surveys has exceeded
80%. However, very few surveys like Pune-Bhigwan(India) have published the diagnostic
break up of all respondents . Some surveys have been more disorder centric rather
than symptom centric .
Though it may not be appropriate to identify individuals,
some have played a seminal role in envisaging and propagating COPCORD. Late Prof
HA Valkenburg (The Netherlands), former Prof
KD Muirden (Australia) and Dr
RD Wigley (New Zealand) were the founding gurus and travelled the length and
breadth of Asia to begin several COPCORD. Prof KD Muirden was the first COPCORD
coordinator. He was succeeded by late Late
Dr John Darmawan (Indonesia) who is credited for galvanizing COPCORD into
an International movement and initiating several measures to standardize COPCORD
surveys. Dr RD Wigley
is the senior most mentor and champion of the World COPCORD movement and is actively
involved in promoting its mission. Prof
Shunle Chen (China) and Prof
Q Zeng have been earlier crusaders to spread COPCORD in China and later in
Asia. Dr
N Khaltaev (WHO) was responsible for bringing the COPCORD data into the folds
of BJD and other initiatives for assessing the global burden of MSK. Prof
Hans Rasker ( The Netherlands) has been an ardent COPCORD supporter and played
a critical role in taking COPCORD into Africa (Egypt). In recent times, Dr
Arvind Chopra (India), Prof
Atiqul Haq (Bangladesh) and Prof
Davatchi (Iran) have played critical COPCORD roles. Prof Davatchi is the current
APLAR COPCORD coordinator. Prof
A Kutzbach (Guatemala) and Dr
Mario Cardiel (Mexico) have recently completed challenging COPCORD in Latin
America. Since 2005, Dr Arvind Chopra has been the COPCORD co-ordinator and responsible
for the current COPCORD fast track model (with a service component) and the recently
revised and proposed CCQ, and forging links
with the BJD.
| Organization,
Structure & Function | |
Though COPCORD has been around for over three
decades, there was no formal organization and structure to administer and execute
and handle budget. Though universally supported by ILAR, and APLAR in particular,
COPCORD has survived through the efforts of individuals rather than international
organizations. In the earlier ILAR organization, COPCORD as a subject was under
the umbrella of its epidemiology committee. Coordinators have been nominated
in the past, both at ILAR and APLAR level (see above). Coordinators have directly
dealt with investigators to provide expert guidance and assistance. Though COPCORD
is extensively published, there is no central doctrine document containing guidelines
and instruments. A core survey questionnaire was constructed by the ILAR at the
launch of COPCORD. The latter has served as a template for future modifications
and versions by the investigators (see above). The core contents of the questionnaire
have remained unchanged in the approach towards RMSK in a community. However,
in several instances, the investigators have taken recourse to their own clinical
sense and expertise. As an example, investigators were not provided with a standard
classification system of RMSK disorders for application. Also, there has been
no standard quality of life assessment in the earlier surveys. The investigators
have had fair laxity to organize the COPCORD survey in the best possible manner
consistent with the local scenario and situation.
The aim has been to
obtain real life community data on RMSK using socioeconomically appealing methods
and techniques. However, the overall methods and methodology used to collect data
in different surveys has ensured fair amount of comparability between COPCORD
surveys around the World.
The current ILAR committee is yet to decide
on the mode of COPCORD functioning. | | | | |
|










































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
_tn.gif){kind=link}